Article Text

Statistics from Altmetric.com
Learning objectives
How to formulate the clinical suspicion of myocarditis.
How to reach the diagnosis of ‘clinically suspected’ and ‘definite (biopsy-proven)’ myocarditis according to the European Society of Cardiology (ESC) 2013 Task Force criteria.
How to interpret non-invasive and invasive diagnostic findings in the context of the heterogeneous clinical presentations of suspected myocarditis.
How to assess prognosis.
Myocarditis represents a challenging diagnosis, mainly because there is no pathognomonic clinical presentation, and the disease may masquerade as a variety of non-inflammatory myocardial diseases. Thus, in the 1996 WHO/International Society and Federation of Cardiology (WHO/ISFC)1 and in the 2007 European Society of Cardiology (ESC) classifications of cardiomyopathies,2 as well as in the 2013 ESC myocarditis Task Force report,3 the disease is defined histologically as an inflammatory disease of the myocardium diagnosed on endomyocardial biopsy (EMB), based upon histological, immunological, immunohistochemical and molecular findings to detect possible infectious causes.1–6 The term inflammatory cardiomyopathy may be used for histologically confirmed myocarditis in association with cardiac dysfunction (box 1).1 Although EMB remains the diagnostic gold standard for myocarditis and it is the only tool that, at present, provides distinction of its aetiological forms,1–6 it is not widely used. This results in lack of certainty in the epidemiological impact and the natural history of the disease. Myocarditis may resolve spontaneously, recur or become chronic, leading about 1/3 of biopsy-proven cases to dilated cardiomyopathy (DCM), death or heart transplantation.7 Traditionally, when the diagnosis was only based upon the histological Dallas diagnostic criteria, myocarditis was considered to be a relatively rare cause of heart failure and/or of sudden cardiac death.8 ,9 Nowadays, the use of highly sensitive immunohistochemical and molecular tools applied to EMB10–18 and of cardiovascular MR (CMR) for non-invasive imaging19–21 suggests that we may be indeed facing the tip of an iceberg, with a substantial underestimation of myocarditis frequency and of its causative role in DCM.
ESC curriculum sections
2.1 History taking and clinical examination
2.2 The ECG
2.3 Non-invasive imaging
2.4 Invasive imaging
2.10 Myocardial diseases
Definitions
Myocarditis (WHO/International Society and Federation of Cardiology (ISFC), European Society of Cardiology (ESC)1–3
Inflammatory disease of the myocardium diagnosed by established histological*, immunohistochemical** and immunological criteria***.
*Established histological Dallas criteria4 defined as follows:
“Histological evidence of inflammatory infiltrates within the myocardium associated with myocyte degeneration and necrosis of non-ischaemic origin”.
**Immunohistochemical criteria, abnormal inflammatory infiltrate3 ,5–6defined as follows:
“≥14 leucocytes/mm2 including up to 4 monocytes/mm2 with the presence of CD3-positive T lymphocytes ≥7 cells/mm2”.
***Immunological criteria and myocarditis aetiology defined as follows3 (see also figure 3):
Viral: histology (Hx) and immunoHx positive (pos), PCR pos for ≥virus
Autoimmune: Hx and immunoHx pos; viral PCR negative (neg); with or without pos cardiac autoantibodies (aabs); exclusion of other known inflammatory causes
Viral and immune****: Hx and immunoHx pos; viral PCR pos; cardiac aabs pos
****N.B. a follow-up endomyocardial biopsy may identify persistent viral myocarditis, resolved myocarditis (Hx and virological), or persistent virus-negative myocarditis, for example, postinfectious autoimmune.
Inflammatory cardiomyopathy and dilated cardiomyopathy (DCM) (WHO/ISFC, ESC)*****1–3
Myocarditis in association with cardiac dysfunction.
*****Involved in the pathogenesis of DCM, includes idiopathic, autoimmune and infectious subtypes.
DCM is a clinical diagnosis characterised by dilation and impaired contraction of the left or both ventricles that is not explained by abnormal loading conditions or coronary artery disease.
******DCM includes idiopathic, familial/genetic, viral and/or immune, alcoholic/toxic subtypes.
Aetiology
Etiopathogenetic agents of myocarditis are shown in table 1. Viral infections are presumed to represent the most common causes in North America and Europe. Viral genomes are detected in the myocardium of a variable proportion of patients using molecular techniques, mainly reverse transcritapse polymerase chain reaction (PCR).7 ,10–18 ,20–22 Parvovirus B19 and human herpes virus 6 (HHV6) are becoming, at least in German series, the most frequently detected virus types, and co-infection is found in a sizable proportion of patients.10 ,13–15 ,18 ,21 ,22 The sensitivity and specificity of EMB for the diagnosis of specific viral infections are unknown and may vary as a function of disease stage, time from onset of clinical symptoms to EMB and variable epidemiology of viral infections in different countries.7 ,10–18 ,20–22 Myocarditis is autoimmune if no infectious agents are identified on EMB and other known causes are excluded (box 1).23 ,24 Autoimmune myocarditis may occur with exclusive cardiac involvement or in systemic autoimmune disorders, in which it is often associated with a bad prognosis,25–29 particularly in Churg–Strauss syndrome,25 ,29 Wegener granulomatosis,26 idiopathic inflammatory myopathies,28 systemic lupus erythematosus27 and is managed with intensified immunosuppression.24–29
Etiopathogenetic agents associated with myocarditis/inflammatory cardiomyopathy
Pathogenesis
Viral myocarditis
The viral pathogenesis of myocarditis associated with parvovirus B19 and HHV6 is at present poorly understood and a subject of intensive research.10 ,30 Recently, parvovirus B19 replication intermediates were found in human acute myocarditis with high viral load but not in DCM; co-infection with other cardiotropic viruses was observed more frequently with HHV6.31 Co-infected patients had higher viral parvovirus B19 load compared with monoinfected patients, suggesting that HHV6 had transactivated parvovirus B19.31 These researchers suggest that parvovirus B19 infection of the human heart may cause the development of an endothelial cell-mediated inflammatory disease and that this is related to both viral load and genotype, in brief that parvovirus B19 infection may be pathogenic only in a subset of patients with myocarditis.10 ,31
Historically, the best studied animal model has been experimentally induced murine Coxsackievirus B3 myocarditis.30–34 In experimental infection with these viruses, only genetically susceptible mouse strains develop acute severe disease as a result of myocyte necrosis due to virus replication; the likelihood of progression to chronic DCM is also higher in susceptible strains, although the severity of acute disease does not always predict the likelihood of progression. Conversely in resistant animals an immune response, mainly mediated by macrophages and T lymphocytes, eliminates the infectious agent within 2 weeks.
Postinfectious and primarily autoimmune myocarditis
In several susceptible mouse strains, enteroviral RNA and inflammation persist in the heart for several weeks, triggering myocardial autoimmune phenomena.30–34 Such mouse strains also develop autoimmune myocarditis (and later on DCM) after immunisation with cardiac myosin, or spontaneously, for example, in the absence of an infectious trigger. In these mice, genetic predisposition is controlled by major histocompatibility complex (MHC) and non-MHC genes,35–44 some associated with type 1 diabetes and other autoimmune diseases.45 ,46 The MHC is the mouse equivalent of the human leucocyte antigen (HLA) complex, which plays a role in human autoimmune myocarditis.44 ,47–51 In the last two decades, the involvement of autoimmunity has been documented in a sizable proportion of myocarditis and inflammatory cardiomyopathy patients, particularly those with a DCM phenotype.23 ,24 ,35–78 Autoimmune diseases in humans fulfil at least two of the major criteria proposed by Witebsky and Rose.79 ,80 In keeping with the findings in other conditions, in myocarditis and in autoimmune DCM there may be familial aggregation48–50 and HLA associations.51 ,81 Other main clinical autoimmune features (box 2) include the findings of mononuclear cell infiltrates, abnormal expression of HLA class II and/or adhesion molecules on cardiac endothelium in the absence of viral genomes (assessed by PCR on EMB) in affected patients and family members,52 ,53 increased levels of serum cytokines and cardiac autoantibodies (aabs) in patients and family members,7 ,23 ,54 ,55 ,57–64 ,67 ,68 ,70 ,72 ,74–78 and response to immunosuppression or immunomodulation.26–29 ,53 ,56 ,73
Fulfilled Rose–Witebsky autoimmune features in myocarditis/dilated cardiomyopathy
Major
Mononuclear cell infiltrates and abnormal human leucocyte antigen (HLA) expression on endomyocardial biopsy in the absence of infectious agents (by PCR) or known inflammatory causes52–53
Serum autoantibodies in patients and in unaffected family members7 ,23 ,54 ,55 ,57–64 ,67–68 ,70 ,72 ,74–78
Autoantibody and/or autoreactive lymphocytes in situ within the affected tissue74
Identification and isolation of autoantigen(s) involved37–46 ,59 ,65–66 ,68 ,71 ,78
Disease induced in animals by immunisation with relevant autoantigen,37–40 ,71 and/or passive transfer of serum, purified autoantibody and/or lymphocytes39 ,54 ,65 ,67–69
Efficacy of immunosuppressive therapy in patients26–29 ,53 ,56 ,73
Minor
Common to all autoimmune disorders
Typical of organ-specific autoimmune disorders
Adapted from Caforio et al.24
A number of cardiac aabs have been found in patients with myocarditis/DCM.7 ,23 ,54 ,55 ,57–64 ,67 ,68 ,70 ,72 ,74–78 A direct pathogenic role by at least some aabs is suggested by (1) demonstration of in vitro functional effects of cardiac aabs isolated from affected patients; (2) induction of the cardiac abnormalities seen in human post-myocarditic DCM by immunisation of animals with defined autoantigens; (3) induction of myocardial pathological changes by transfer of immune components from one experimental animal to another; (4) demonstration of improved cardiac morphology and function by specific removal of aabs by immunoabsorption in animals (box 2). For example, a study suggests that anticardiac myosin aabs induced by immunisation of rats against cardiac myosin cross-react with cardiac membrane beta1-adrenergic receptors and enhance cAMP-dependent protein kinase A activity in myocytes.39 Passive transfer of purified aabs from cardiac myosin-immunised rats results in IgG deposits and increases myocyte apoptosis in the heart, leading to a cardiomyopathic phenotype in recipients.39
Clinical presentations in biopsy-proven myocarditis
In myocarditis, cardiac signs and symptoms are heterogeneous and lack specificity, depending on the degree of myocardial inflammation and ventricular dysfunction, and may be subtle; thus, the disease may be unrecognised.3 ,7–12 ,16–18 ,20–22 ,24 Myocarditis should be suspected in a previously asymptomatic young subject with few coronary artery disease (CAD) risk factors who, days or weeks after a presumed respiratory or gastrointestinal viral syndrome with or without increased systemic inflammatory markers and fever, develops dyspnoea or orthopnoea, or palpitations, or effort intolerance/malaise, or heart failure, or chest pain (which may be pleuritic if concomitant pericarditis is present) with or without cardiac troponin I or T (cTNI or cTNT) release and unobstructed coronary arteries at coronary angiography.3 ,7–12 ,16–18 ,20–22 ,24 ,82 ,83 Biopsy-proven myocarditis may also present with arrhythmia, including syncope or aborted sudden death,3 ,7–12 ,16–18 ,20–22 ,84 subacute or chronic heart failure, or new-onset acute heart failure and/or cardiogenic shock.3 ,7–12 ,16–18 ,20–22 ,24 Myocarditis may also accompany or cause peripartum cardiomyopathy3 ,7 or Takotsubo cardiomyopathy.85 Fulminant myocarditis has been described as having viral prodromes within 4 weeks before cardiac symptoms, a distinct onset of unexplained heart failure, haemodynamic compromise and, in general, a good prognosis.86 Since myocarditis can simulate many non-inflammatory pathologies, any other cause (eg, valve heart disease, pericardial constriction, CAD) should be excluded.
ECG and echocardiographic findings in biopsy-proven myocarditis
Similar to the clinical presentation, ECG findings are also not specific or sensitive for myocarditis including all types of ‘idiopathic’ atrial or ventricular tachyarrhythmias or bradyarrhythmias, P-Q segment depression and/or repolarisation abnormalities.3 ,7–12 ,16–18 ,20–22 ,24 ,84 Still, some ECG changes are suggestive for myocarditis: ST-T segment elevation is more concave (convex in ischaemia) and diffusely present over the precordial leads, without reciprocal changes. PR-depression is frequently present in pericarditis associated with myocarditis, but is rare in cardiac ischaemia. Q-waves are uncommon in myocarditis. T-wave inversion generally occurs after complete ST-T normalisation in myocarditis, but usually takes place while the ST-segment is still elevated after myocardial infarction.
Echocardiography defines morphology and biventricular function, but it is not specific. It may be normal or similar to DCM. Pericardial effusion may be present, as well as segmental wall motion abnormalities.87 ,88 Apical LV aneurisms suggest Chagas's disease. In fulminant myocarditis, there may be a slight increase in LV wall thickness and a mildly dilated severely hypokinetic ventricle.87 Echocardiography is helpful in ruling out some non-inflammatory causes of cardiac signs and symptoms or associated conditions, for example, valve disease. In addition, it provides non-invasive morpho-functional imaging at presentation and during follow-up since temporal changes in terms of systolic function, chamber size and thickness may occur very quickly in myocarditis requiring repeat echocardiographies.
Nuclear and CMRI
Overall, 111indium antimyosin antibody and gallium-67 nuclear imaging are rarely used (limited availability of tracers, poor spatial resolution, radiation issues, low diagnostic accuracy), although the recent development of novel (molecular) nuclear tracers appears promising at least in animal models.89 ,90 One exception is represented by gallium-67 scintigraphy and positron emission tomography (PET) with fluorodeoxyglucose in the acute phase and in the follow-up of cardiac sarcoidosis.90
CMRI defines morphology and biventricular function of the heart and provides tissue characterisation.3 ,19–22 ,91 The “International Consensus Group on CMR Diagnosis of Myocarditis” suggested the combined use of three different CMR techniques, the so-called Lake Louise criteria.19 Myocardial oedema is assessed on T2-weighted CMR images, hyperaemia/capillary leak on myocardial early gadolinium enhancement ratio and necrosis/fibrosis on late gadolinium enhancement (LGE). LGE is typically subepicardial, localised in inferolateral and less frequently in anteroseptal LV segments, and may be focal or diffuse in distribution. The best overall diagnostic accuracy (78%) is found by the combination of all three tissue-based CMR parameters, but correlative data with EMB are still based on low numbers. CMR does not differentiate specific inflammatory cells (eg, lymphocytes, giant cells) or viral from non-viral myocarditis.3 ,19–22 ,91 According to the 2013 ESC Task Force, in clinically stable patients, CMR, if available, can strengthen the clinical suspicion of myocarditis before EMB; in life-threatening presentations, EMB should not be postponed.3 ,92 ,93 CMR could replace EMB in the follow-up of diagnosed patients when there is no evidence of viral infection on EMB; on the opposite, if the first EMB is in keeping with viral myocarditis, a second EMB should be required to check the viral clearance from the myocardium.3
Diagnostic role of biomarkers
Inflammatory markers
Erythrocyte sedimentation rate and C reactive protein levels are not raised in the majority of patients with biopsy-proven myocarditis; conversely, these are often increased in acute pericarditis.3 ,7
Troponin and brain natriuretic peptides
Cardiac troponins do not differentiate ischaemic from inflammatory myocyte injury, may be raised in several other conditions and when normal do not exclude myocarditis.3 ,7 ,17 Similar limitations probably apply to cardiac hormones such as brain natriuretic peptides, circulating cytokines, markers related to extracellular matrix degradation and new biomarkers such as pentraxin 3, galectin 3 and growth differentiation factor 15.3
Viral serology
Positive viral serology does not imply active myocardial infection. The prevalence of circulatory IgG antibodies to cardiotropic viruses in the general population is high in the absence of viral heart disease.30 ,34 ,94 In addition, infection with non-cardiotropic enteroviruses may cause an antibody response that is indistinguishable from the response to cardiotropic viruses,30 ,34 ,94 and in a recent study, there was no correlation between virus serology and EMB findings.95 Thus, viral serology is not recommended by the ESC 2013 Task Force, except for hepatitis C, rickettsial phase 1 and phase 2, Lyme disease in endemic areas as well as HIV serologies in high-risk patients and in certain populations at high prevalence of infection.3
Serum cardiac aabs
In patients with myocarditis/idiopathic DCM and of their symptom-free relatives, circulating heart-reactive aabs are directed against multiple antigens, some of which are strictly expressed in the myocardium (eg, organ-specific for the heart), others expressed in heart and skeletal muscle (eg, muscle-specific), as shown in figure 1.7 ,23 ,54 ,55 ,57–64 ,67–68 ,70 ,72 ,74–78 Distinct aabs have also different prevalence in disease and normal controls (eg, the organ-specific and cross-reactive 1 type of antiheart aabs shown figure 1 are disease-specific for myocarditis/DCM, some of the muscle aabs are not).7 ,23 ,54 ,55 ,57–64 ,67–68 ,70 ,72 ,74–78 Aabs of IgG class, which are shown to be cardiac and disease-specific for myocarditis/DCM, can be used as autoimmune markers for identifying patients in whom immunosuppression and/or immunomodulation therapy may be beneficial and their relatives at risk.3 ,7 ,24 ,47–49 ,57–59 Some aabs may have a functional role and thus have an impact on the patients’ prognosis.39 ,47 ,54 ,55 ,60 ,63–64 ,66–68 ,75–78 The ESC Task Force recommended to assess sera with clinically suspected or definite myocarditis for cardiac aabs, using one (or more) of the published tests, according to specific centre expertise, preferably disease-specific aabs.3

Antiheart aabs (AHA) patterns by indirect immunofluorescence test. Organ-specific AHA and antinuclear aabs (ANA) pattern. (A) On human heart tissue: cytoplasmic diffuse staining of cardiac myocytes (organ-specific AHA pattern) and diffuse staining of the nuclei (non-organ-specific ANA pattern) (×200); (B) (×400) on human skeletal muscle tissue: negative for AHA, positive for ANA. Partially organ-specific (or cross-reactive 1) AHA pattern. (C) On human heart tissue: strongly positive fine striational pattern (×400); (D) on human skeletal muscle: weak positive fine striational pattern (×400). Entirely cross-reactive (or cross-reactive 2) AHA pattern. (E) On human heart tissue: strong positive striational pattern (×400); (F) on human skeletal muscle: strongly positive (×400). Negative AHA control serum pattern. (G) On human heart tissue: negative (×400); (H) on human skeletal muscle: negative (×400).
Clinically suspected myocarditis: the 2013 Task Force criteria
To aid the clinician in the identification of myocarditis, the ESC Myocarditis Task Force has introduced new rigorous criteria for clinically suspected myocarditis using the combination of a plausible clinical presentation and of diagnostic criteria from different categories, as well as exclusion of known non-inflammatory causes, for example, CAD, that could explain the syndrome.3 (figures 2 and 3, key points 1–2). These criteria were proposed to better refine the clinical and non-invasive diagnosis of myocarditis also in centres that do not routinely perform EMB.

Clinical presentations and diagnostic European Society of Cardiology 2013 Task Force criteria for clinically suspected myocarditis. CMR, cardiac MR; LGE, late gadolinium enhancement.

Diagnostic work-up and aetiology-based management in myocarditis according to the European Society of Cardiology 2013 Task Force criteria. Aab, cardiac autoantibody, EMB, endomyocardial biopsy.
The 2013 ESC Task Force criteria of clinically suspected myocarditis: key point 1
Clinically suspected myocarditis is defined by the presence of >1 clinical presentation (with or without ancillary findings) and >1 diagnostic criteria from different categories, in the absence of
Angiographically detectable CAD (coronary stenosis ≥50%).
Known pre-existing cardiovascular disease or extra-cardiac causes that could explain the syndrome (eg, valve disease, congenital heart disease). Suspicion is higher with higher number of fulfilled criteria.
If the patient is asymptomatic, >2 diagnostic criteria should be met.
Medical history should focus on
Family history of DCM, other cardiomyopathy, sudden cardiac death, autoimmune disease.
Patients’ history: recent (days to 2 weeks) upper respiratory or gastrointestinal suspected viral syndrome, allergy, other autoimmune diseases, previous clinically suspected or proven myocarditis, heavy alcohol intake, assumption of drugs and toxic substances (eg, cocaine), vaccines, travel to places where specific cardiotropic infection is possible or endemic (eg, Brazil, Argentina and Chile for Chagas’s disease), proximity with domestic animals, conventional coronary risk factors, etc. The aim is search as well as exclude possible treatable causes (eg, drug-related toxicity or hypersensitivity).
The 2013 ESC Task Force criteria of clinically suspected myocarditis: key point 2
Clinical presentations3 include ≥1 of the following:
Acute coronary syndrome-like, with or without normal global or regional LV and/or RV dysfunction on echocardiography or CMR, with or without increased troponin (Tn)T/TnI (that may have a time course similar to acute myocardial infarction or a prolonged and sustained release over several weeks or months).
New onset or worsening heart failure in the absence of CAD and known causes of heart failure.
Chronic heart failure, with heart failure symptoms (with recurrent exacerbations) of >3 months duration, in the absence of CAD and known causes of heart failure.
Life-threatening condition (including life-threatening arrhythmias and aborted sudden death, cardiogenic shock, severely impaired LV function), in the absence of CAD and known causes of heart failure.
Diagnostic criteria3 include ≥1 of the following features from categories I to IV:
Electrocardiogram (ECG)/Holter/stress test features
Newly abnormal 12-lead ECG and/or Holter and/or stress testing, any of the following (see also figure 2): I to III degree atrioventricular block, or bundle branch block, ST/T-wave change (ST elevation or non-ST elevation, T-wave inversion), sinus arrest, ventricular tachycardia or fibrillation and asystole, atrial fibrillation, reduced R-wave height, intraventricular conduction delay (widened QRS complex), abnormal Q waves, low voltage, frequent premature beats, supraventricular tachycardia.
Myocardiocytolysis markers (elevated cardiac troponins).
Functional and structural abnormalities on cardiac imaging (echo/angio/CMR)
New, otherwise unexplained LV and/or RV structure and function abnormality (including incidental finding in apparently asymptomatic subjects): any of those in figure 2.
Tissue characterisation by CMR
Oedema and/or LGE of classical myocarditic pattern (according to Lake Louise criteria).19
Diagnosis of definite (biopsy-proven) myocarditis by ESC 2013 Task Force criteria
In patients fulfilling the diagnostic criteria for clinically suspected myocarditis, the ESC Myocarditis Task Force recommends selective coronary angiography and EMB, including conventional histology, as well as immunohistochemistry and PCR detection of infectious agents3 ,6 (box 1). To increase the diagnostic sensitivity of histology, immunohistochemistry using a panel of monoclonal and polyclonal antibodies, including anti-CD3, T lymphocytes; anti-CD68, macrophages; and anti HLA-DR, is recommended for the identification and characterisation of the inflammatory infiltrate and for the detection of HLA-DR upregulation on EMB tissue sections as marker of infectious-negative autoimmune myocarditis where immunosuppression may be considered.3 ,6 Other immunofluorescence stains used to define humoral rejection in heart transplant EMB, such as C3d and C4d, may provide additional markers of immune activation in patients with inflammatory cardiomyopathy; a limitation of these stains is that they require frozen material.3 ,6 This recommendation also applies to patients with an acute coronary syndrome-like presentation, not included in the American Heart Association/American College of Cardiology/Heart Failure Society of America scientific statement on EMB9 . The Task Force gave this recommendation based upon the following considerations (see also key point 3): (a) If EMB is performed by experienced teams, its complication rate is low and similar to that of standard coronary angiography (0–0.8).3 ,73 ,92 ,93 (b) EMB confirms the diagnosis of myocarditis, and at present it is the only tool to identify the underlying aetiology and the type of inflammation that imply different treatments and prognosis3 ,6 ,7 ,18 ,24 ,94 (figures 3 and 4). (c) EMB is the basis for safe (infection negative) immunosuppression.3 ,73
{kind=link}
{kind=link}
{kind=link}
{kind=link}
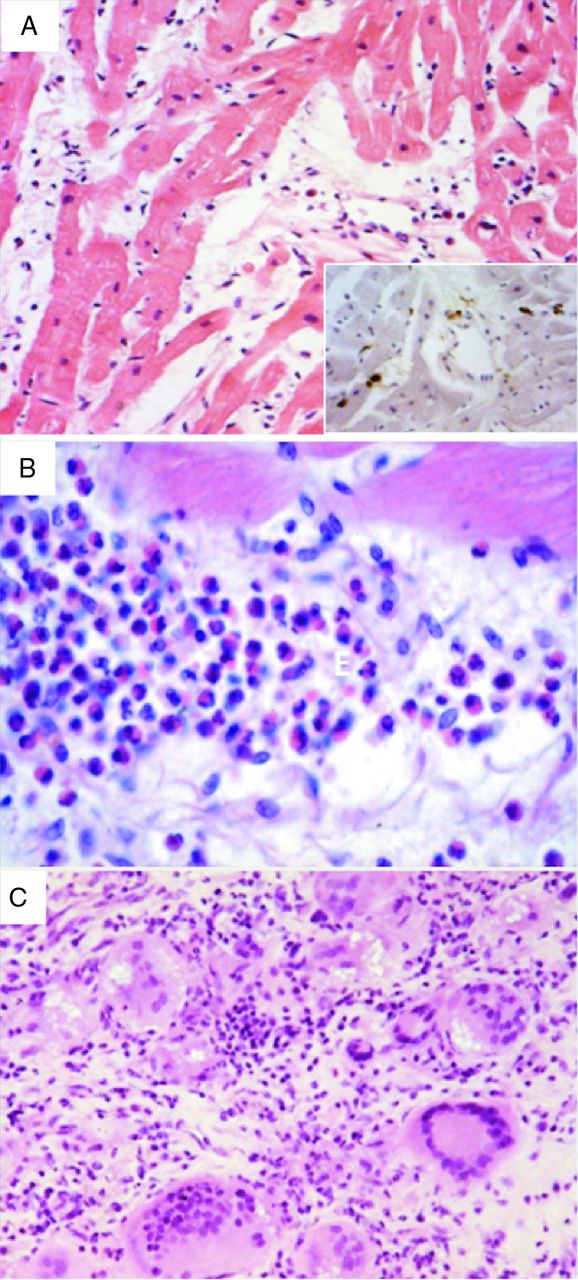
Pathological example of lymphocytic myocarditis (A), eosinophilic (B) and giant cell myocarditis (C) on endomyocardial biopsy. (H&E stain; inset in (A) CD3 stain, lymphocytic marker) (modified from Basso et al94).
Diagnosis of definite (biopsy-proven) myocarditis: key point 3
EMB, including conventional histology (Dallas criteria), as well as immunohistochemistry and PCR detection of infectious agents is the gold standard for diagnosis of myocarditis.
Absence of infectious agents identifies immune-mediated myocarditis, either primary or postinfectious, if an infectious agent had been identified on a previous EMB, and is the basis for safe (infection negative) immunosuppression.
EMB is essential to identify specific myocarditis types (eg, giant cell, eosinophilic, sarcoidosis), which imply different treatments and prognosis.
EMB provides differential diagnosis from diseases that may mimic myocarditis (arrhythmogenic RV cardiomyopathy, Takotsubo cardiomyopathy, peripartum cardiomyopathy, infiltrative/storage disorders, cardiac masses).
If EMB is performed in experienced centres, its complication rate is similar to that of standard coronary angiography.
EMB may be taken from the right or from the LV according to centre and operator preference and expertise. Antiplatelet or anticoagulation strategy for LV EMB may be different among centres.
Clinical presentation of specific forms of myocarditis
Non-viral, infectious myocarditis
The spirochete Borrelia burgdorferi causes Lyme disease, which can result in a broad spectrum of presentations, from asymptomatic, first-degree to advanced heart block or to transient life-threatening myocardial dysfunction.96 Advanced heart block may require temporary pacing; it resolves within 1 week in most cases. Tripanozoma cruzi (Chagas’s disease), a common cause of myocarditis/DCM in South America, with a suggested postinfectious autoimmune component, has an acute phase of mild febrile course and a prolonged (up to 30 years) symptom-free latent phase.97 Systolic and diastolic heart failure, ventricular aneurisms, arrhythmias and cardiac autonomic dysfunction may be present. Toxoplasma gondii associated and fungal myocarditis has been mostly observed among seronegative cardiac transplant recipients of seropositive donors and in other immunodeficient populations with multiple opportunistic infections, particularly HIV.24
Giant cell myocarditis, sarcoidosis and myocarditis in extra-cardiac autoimmune disease
Giant cell myocarditis, the prototype of autoimmune myocarditis, is a rare but devastating disease, presents as other forms of myocarditis, but is characterised by a rapid and severe downhill course, despite optimal medical care.3 ,6 ,7 ,9 ,17 ,56 ,84 It may be associated with a variety of autoimmune disorders and may recur in the native heart following recovery and in the donor heart following transplantation with up to 25% rate of recurrence; relapse in both conditions usually responds to intensified immunosuppression.3 ,6 ,7 ,9 ,17 ,56 ,84 Sarcoidosis, a systemic granulomatous disease of unknown aetiology and suspected immune origin, may present initially or predominantly with myocardial involvement, mimicking arrhythmogenic cardiomyopathy; ventricular septum and conduction system involvement can lead to bradyarrhythmia or tachyarrhythmia and sudden cardiac death.9 ,90 Myocarditis in connective tissue diseases, and in other immune-mediated systemic diseases (box 1), includes a range of clinical expressions, from conduction diseases to DCM.25–29
Myocarditis in rheumatic heart disease
Although rheumatic fever (RF) remains a leading cause of acquired cardiopathy on a global scale, well-conducted recent studies on biopsy-proven acute or chronic rheumatic myocarditis are lacking because RF is rare in Europe and the USA; most of the literature on this subject date back to the 1950s. It is unclear whether or not myocarditis in RF can be defined as infectious or postinfectious autoimmune according to the 2013 Task Force criteria. The histological finding of Aschoff bodies is the hallmark of rheumatic inflammation in the heart.3 ,6 ,24 Rheumatic myocarditis is thought to be a component of acute rheumatic carditis, which also includes pericarditis and valvulitis. In acute rheumatic heart disease, histological analyses have shown the presence of dense valvular mainly CD4+ inflammatory cell infiltrates and Aschoff nodules in the myocardium.3 ,6 ,24 In addition, CD4+ and CD8+ infiltrating T-cell clones recognised streptococcal M peptides and cardiac tissue proteins, suggesting that molecular mimicry may be the mechanism responsible for postinfectious autoimmunity to heart structures.3 ,6 ,24 However, in acute rheumatic myocarditis, histopathology reveals no necrosis and for this feature there are authors who have questioned that rheumatic myocarditis exists.6 ,24 Because acute rheumatic myocarditis is frequently asymptomatic, its diagnosis is difficult and requires a high-suspicion rate.3 ,6 ,24 ,98 Rheumatic patients with acute myocarditis often present mild symptoms such as tachycardia or mild worsening of heart failure, frequently attributed to worsening of the valvular heart disease or another cause of decompensation, such as volume or salt overload. The diagnosis of acute rheumatic myocarditis requires the use of multiple imaging techniques. An echocardiography can reveal mild to moderate pericardial effusion (rarely pericardial effusion or even pericardial tamponade). Transoesophageal echocardiography can sometimes show small multiple vegetations on the edge of native valves, representing the rheumatic verrucae that characterise the acute phase of the disease. The 12-lead ECG may reveal a first-degree atrioventricular heart block, which is a sign of myocarditis, but this is not very sensitive. Imaging techniques that highlight inflammation in the heart may be useful, for example, gallium-67 myocardium scintigraphy.3 ,6 ,24 ,98 A good correlation has been shown between a positive scintigraphy and EMB for the diagnosis of active rheumatic myocarditis. PET-CT is currently being evaluated and appears to have a better sensitivity than the gallium scan.3 ,6 ,24 ,98 In conclusion, acute rheumatic myocarditis is a difficult diagnosis that should be considered in any patient, including patients who have just undergone valve surgery, with rheumatic valvular heart disease who present with a sudden worsening of heart failure symptoms or rapid-onset ventricular dysfunction, particularly if the patient is not on secondary prophylaxis for RF.
Toxic and hypersensitivity myocarditis
Hypersensitivity myocarditis, probably the most common form of drug-induced cardiac toxicity, is unpredictable and not related to drug dosage. Non-specific skin rash, malaise, fever and eosinophilia may suggest the diagnosis, but are absent in many cases.6 ,24 On the other hand, a direct cardiac toxicity is dose-dependent, may be reversible and is often potentiated by other antineoplastic treatments, such as radiotherapy.
Paediatric myocarditis
Myocarditis is considered a frequent cause of a new-onset DCM phenotype in children, with small studies reporting high rates of recovery of LV function. Most published data are either retrospective or observational and often based on administration registries. In addition, diagnosis is biopsy-proven in a minority of patients. In a recent multi-institutional paediatric registry from the USA, children with biopsy-confirmed or probable myocarditis had similar proportions of death, transplantation and echocardiographic normalisation 3 years after presentation and better outcomes than those of children with idiopathic DCM.99 In children with myocarditis who had impaired LV ejection at presentation, rates of echocardiographic normalisation were greater in those without LV dilation and in those with greater septal wall thickness at presentation99 A nation-wide survey in Japan collected 169 clinically suspected cases, with an incidence of 43.5 cases/year and 0.26 cases/100 000.100 Major clinical presentations at onset were congestive heart failure, refractory arrhythmia and syncope in 70, 37 and 17 patients, respectively, 64 cases were fulminant, 89 acute and 8 chronic. Mechanical support seemed effective and life-saving. Survival was 73%, and two-thirds of survivors had no sequelae. An EMB was performed in only 33% of cases; therefore, aetiology-specific markers could not be defined.100 In another survey from the USA, 514 cases of clinically suspected acute myocarditis were identified from April 2006 to March 2011 using the Pediatric Health Information System database.101 Ninety-seven patients (18.9%) received extracorporeal membrane oxygenation (ECMO), 22 (4.3%) received ventricular assist device (VAD), 21 (4.1%) underwent heart transplantation and 37 (7.2%) died. Of the 104 patients who received ECMO or VAD, 17 (16.3%) had heart transplantation, 25 (24%) died and 62 (59.6%) showed recovery of myocardial function. Although ECMO, VAD and vasoactive medications were independently associated with increased mortality/transplantation, it was concluded that ECMO or VAD may be successful strategies in supporting patients until resolution of cardiac dysfunction or as a bridge to transplant because 76% of this high-risk cohort were successfully bridged to transplant or recovery. Again EMB was performed in a minority.101 One study suggested that a routine performance of EMB in critically ill children with DCM is useful to identify those with myocarditis who do not need heart transplantation.102 More prospective data are needed to clarify the prognostic impact of aetiology and disease stage in paediatric myocarditis.
Summary and conclusion
The ESC 2013 Task Force consensus document recommends a systematic consideration of EMB in patients with stringent criteria for clinically suspected myocarditis that combine clinical presentation and non-invasive diagnostic features.3 However, EMB should not be limited to standard histology (Dallas criteria), but include immunohistochemistry, and molecular analysis for infectious agents and should be performed by experienced teams. The rationale for suggesting such in-depth diagnostic effort is the availability of a wide range of immunosuppressive17 ,24 ,56 ,73 and immunomodulatory therapeutic options3 ,17 ,24 ,77 for infection-negative patients, which, in principle, as seen in extra-cardiac autoimmune disease, and in the available clinical studies, could be beneficial to stop or control the chronic cardiac tissue injury mediated by the immune system leading to irreversible fibrosis and burned out DCM. For some specific forms of myocarditis, immunosuppression is established,25–29 ,3 ,6 ,7 ,9 ,17 ,56 ,84 ,90 ,103 but more evidence-based data from multicentre randomised controlled trials in the majority of patients with infection-negative biopsy-proven myocarditis are needed to define indications, efficacy on morbidity and mortality, drug regimens and length of treatment. In addition, the same diagnostic work-up will make it feasible to test future antiviral treatments in infection-positive patients.104 ,105
Key messages
Clinically suspected myocarditis, according to the European Society of Cardiology (ESC) 2013 Task Force criteria, is defined by the presence of >1 clinical presentation (with or without ancillary findings) and >1 diagnostic criteria from different categories, in the absence of:
Angiographically detectable coronary artery disease (coronary stenosis ≥50%).
Known pre-existing cardiovascular disease or extra-cardiac causes that could explain the syndrome (eg, valve disease, congenital heart disease). Suspicion is higher with higher number of fulfilled criteria.
If the patient is asymptomatic, >2 diagnostic criteria should be met.
The ESC 2013 Task Force document recommends consideration of endomyocardial biopsy (EMB) in all cases of clinically suspected myocarditis.
The diagnosis of definite myocarditis according to the ESC 2013 Task Force criteria is based upon EMB confirmation, including conventional histology (Dallas criteria), as well as immunohistochemistry and PCR detection of infectious agents.
Absence of infectious agents identifies immune-mediated myocarditis, either primary or post-infectious if an infectious agent had been identified on a previous EMB, and is the basis for safe (infection negative) immunosuppression.
EMB is essential to identify specific myocarditis types (eg, giant cell, eosinophilic, sarcoidosis), which imply different treatments and prognosis.
EMB provides differential diagnosis from diseases that may mimic myocarditis (arrhythmogenic RV cardiomyopathy, Takotsubo cardiomyopathy, peripartum cardiomyopathy, infiltrative/storage disorders, cardiac masses).
The 2013 ESC Task Force consensus document gives specific guidance for aetiology-directed treatment in the diverse etiopathogenetic subsets of definite myocarditis, particularly in relation to immune-mediated forms.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Acknowledgments
CB is supported by the Registry for Cardio-cerebro-vascular pathology, Veneto Region, Venice, Italy.
References
- ↵
- ↵Current classification of the cardiomyopathies endorsed by the ESC Working group on myocardial and pericardial disease.
- ↵Expert consensus paper endorsed by the ESC Working group on myocardial and pericardial disease that introduces new diagnostic criteria for clinically suspected and definite myocarditis and provides clinical guidance on work-up, management and therapy. It includes suggested technical requirements for immunohistochemistry and molecular analysis.
- ↵Historical paper setting up the Dallas histological criteria for myocarditis.
- ↵
- ↵Recent landmark pathologists’ consensus paper on endomyocardial biopsy and its diagnostic role, technical requirements, strengths and limitations. It includes new immunohistological and molecular virological analysis applied to endomyocardial biopsy.
- ↵
- ↵
- ↵Scientific statement on the role of endomyocardial biopsy in cardiovascular disease. It does not include indications in relation to new immunohistological and molecular virological analysis applied to endomyocardial biopsy.
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵First report which describes the association of progressive cardiac dysfunction with viral persistence at a follow-up endomyocardial biopsy.
- ↵First report describing a high prevalence of adenovirus in paediatric biopsy-proven myocarditis.
- ↵
- ↵This study shows that immunohistochemical findings on endomyocardial biopsy predict a bad outcome in myocarditis.
- ↵Consensus paper with the first description and introduction of the Lake Louise criteria for the CMR diagnosis of myocarditis that are currently used.
- ↵Interesting paper showing that when assessed in biopsy-proven myocarditis CMR has lower sensitivity, even using Lake Louise criteria, than that reported in ref. 19 according to the type of clinical presentation, being lower in heart failure and in arrhythmic than in infarct-like presentations. Thus, according to the authors’ findings a negative CMR does not always rule out biopsy-proven acute myocarditis and should not preclude the use of endomyocardial biopsy in clinically suspected cases. This observation is in keeping with ESC 2013 Task Force recommendations set in ref. 3.
- ↵Paper showing, similar to ref. 20, that CMR findings may be less sensitive than endomyocardial biopsy for myocarditis diagnosis.
- ↵
- ↵
- ↵Recent review focusing on immune-mediated myocarditis from clinical presentation to treatment.
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵Recent extensive review on viral myocarditis from experimental models to clinical studies dealing with molecular diagnosis.
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵First report showing increased frequency of serum cardiac-specific autoantibodies in apparently symptom-free relatives of patients with dilated cardiomyopathy.
- ↵First prospective follow-up study in relatives of dilated cardiomyopathy patients showing that a positive serum cardiac autoantibody test at baseline predicts development of dilated cardiomyopathy at 5-year follow-up in subjects with and without minor echocardiographic abnormalities at baseline. This study shows that immune-mediated dilated cardiomyopathy has a long pre-clinical phase and that the autoimmune serology test provides an non-invasive marker of pre-clinical disease.
- ↵
- ↵Recent landmark large multicenter European genome-wide association study showing that, without a pre-specified hypothesis, HLA is a risk locus for dilated cardiomyopathy, in keeping with the autoimmune paradigm.
- ↵Paper showing that apparently healthy relatives of patients with dilated cardiomyopathy have features of immune activation at endomyocardial biopsy at a very early, pre-clinical stage, and that dilated cardiomyopathy is the end result of a subtle long-lasting myocardial inflammatory process in genetically predisposed subjects.
- ↵
- ↵Recent study proving new evidence by classical passive transfer experiment for direct pathogenic role of cardiac autoantibodies in human myocarditis.
- ↵
- ↵Paper showing the usefulness of intensive immunosuppression for giant cell myocarditis.
- ↵
- ↵
- ↵Paper showing that cardiac-specific autoantibodies in patients with dilated cardiomyopathy, similar to the murine model of experimental autoimmune myocarditis, recognise α and β cardiac myosin heavy chain isoforms as major autoantigens.
- ↵
- ↵
- ↵Paper showing that antibodies against the β1-adrenoceptor, another relevant autoantigen in dilated cardiomyopathy, may have functional positive chronotropic effect.
- ↵Paper showing for the first time the feasibility of immunoadsorption in dilated cardiomyopathy patients to eliminate potentially cardiotoxic cardiac autoantibodies.
- ↵
- ↵
- ↵Paper showing that cardiac autoantibodies against troponin I are responsible for the development of dilated cardiomyopathy in PD-1-deficient mice, suggesting that in a genetically predisposed animal dilated cardiomyopathy is an autoantibody-mediated disease.
- ↵
- ↵Study showing that in another experimental model also antibodies against β1-adrenergic receptor are responsible for autoimmune dilated cardiomyopathy.
- ↵
- ↵
- ↵
- ↵
- ↵First randomised monocentric study showing the efficacy of immunosuppressive therapy with azathioprine and steroids in patients with virus-negative inflammatory cardiomyopathy.
- ↵
- ↵Study demonstrating functional activity of autoantibodies against the beta1 adrenoceptor from patients with dilated cardiomyopathy in vitro.
- ↵
- ↵
- ↵
- ↵Landmark study setting new diagnostic criteria for defining autoimmune diseases, with a modification of historical Witebsky's postulates.
- ↵
- ↵Recent meta-analysis suggesting an association of HLA-DR4 antigen and dilated cardiomyopathy.
- ↵Important study showing the association of parvovirus B19 infection, virus which infects endothelial cells, and myocarditis with pseudo-infarct presentation.
- ↵Interesting study suggesting that parvovirus B19, which infects cardiac endothelial cells, in patients with myocarditis and pseudo-infarct presentation may induce coronary vasospasm and consequently chest pain symptoms.
- ↵Important study describing an unexpectedly high frequency of cardiac sarcoidosis and giant cell myocarditis as causes of unexplained atrioventricular block in young and middle-aged adults, suggesting that these two potentially lethal but treatable forms of myocarditis, regarded to be rare, may be under-recognised.
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵Important study describing the higher yield of etiological diagnosis in patients with myocardial infarction and normal coronary arteries using both CMR and endomyocardial biopsy.
- ↵
- ↵
- ↵
- ↵Important study reporting the lack of correlation between viral serology and biopsy-proven viral myocarditis. This study has had an impact on the recommendations by the ESC Task Force (ref 3) in relation to application of viral serology in clinically suspected myocarditis. It is not recommended any more in all patients, but only in selected cases (see text).
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵One of the few recent Cardiology Society guidelines for myocarditis, issued by the Japanese Circulation Society.
- ↵
- ↵Single centre experience on the application of interferon-beta treatment for biopsy-proven enteroviral persistence in inflammatory cardiomyopathy, describing virus clearance and improvement of left ventricular function.
Footnotes
Contributors Substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data: RM and CB. Drafting the work or revising it critically for important intellectual content and final approval of the version published: RM CB and SI.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.